
Implementation of a randomized mobile-technology lifestyle program in individuals with nonalcoholic fatty liver disease

Patient population
The design of this study was modeled off of our initial pilot intervention previously described7. We prospectively enrolled 70 adult patients with a diagnosis of NAFLD from our hepatology outpatient clinic in Ann Arbor, Michigan between April 2019 and March 2020 with follow-up through August 2020. To meet diagnostic criteria for NAFLD, a participant was required to have imaging [ultrasound (US), Vibration controlled transient elastography (VCTE) (Fibroscan, Echosens), computed tomography (CT), or Magnetic Resonance Imaging (MRI)] demonstrating steatosis within the prior 24 months or a liver biopsy noting hepatic steatosis within the prior 36 months, with no or minimal weight loss (< 5%) since those tests. This testing window was selected to minimize the need for repeating previously performed tests to qualify for entry into the study. Ten subjects had imaging or biopsy completed 6-months or more prior to enrollment with the remaining having testing completed within 6-months prior to enrollment. Patients with any other additional cause of chronic liver disease such as hepatitis B or C were excluded. Alcohol assessment was conducted based on chart review and participant response to query during screening visit. Patients who reported > 14 drinks per week for males or > 7 drinks per week for females at time of their screening visit or with any prior history of alcohol use disorder were excluded. All participants were required to be able to participate in a walking program and basic nutritional interventions (able to follow a Mediterranean or low carbohydrate diet). Those with severe medical co-morbidities (i.e., severe cardiopulmonary disease, severe musculoskeletal disease, uncontrolled diabetes, active malignancy), hepatic decompensation, prior liver transplant, or hepatocellular carcinoma were excluded. Participants with compensated cirrhosis were eligible for enrollment given the overall systemic health benefits of healthier lifestyle habits in addition to data supporting the role of lifestyle interventions in this population in reducing risk of clinical decompensation including reductions in degree of portal hypertension8. Individuals receiving medications that may cause hepatic steatosis or weight reduction, and those who had plans for bariatric procedures or enrollment in other structured lifestyle programs were also excluded. Participants were required to have access to a computer or a smartphone with internet connection.
Data collection
At enrollment we obtained data on demographics, medical comorbidities, vital signs and anthropometrics, laboratory studies (up to 6 months from time of enrollment), physical function and frailty measures, hepatic imaging and several survey measures. Physical function was assessed using the 6-minute walk test (6MWT). The 6MWT is an efficient, low-cost method to assess functional exercise capacity that has been validated in individuals with chronic liver disease9. Frailty was assessed using hand grip strength via dynamometry according to established protocols by trained research staff. Three measurements were made with each hand and the dominant hand was noted. VCTE liver stiffness (LSM) and controlled attenuation parameter (CAP) measurements were obtained at baseline unless results of VCTE performed within 6 months prior to enrollment were available and participant did not have ≥ 5% weight loss since that exam.
Physical activity was assessed using the validated short-version International Physical Activity Questionnaire (IPAQ)10. Dietary assessment was conducted using the Starting the Conversation survey which has been used extensively as a concise measure of healthy eating11. This is an eight question tool that assessed the frequency of intake of fast food, vegetables, fruits, sugar-sweetened beverages, low-fat and lean proteins, chips and crackers, desserts/other sweets and margarine/butter/meat fat. Each response is scored from 0 to 2 for a maximum of 16 points, with higher scores indicating unhealthy dietary habits. Health-related quality of life (HRQOL) measures were obtained using the Chronic Liver Disease Questionnaire-NAFLD (CLDQ-NAFLD)12. This instrument consists of 36 items over six domains: fatigue, abdominal symptoms, emotional function, systemic symptoms, activity, and worry. Each question requires a response on a Likert-scale from 1–7 to indicate “all of the time” to “none of the time”. Responses to these items are averaged to give a summary score between 1 and 7 with higher scores indicating higher HRQOL. Motivation to change health behaviors was evaluated using the validated Stages of Change questionnaire13. This model categorizes readiness to change health behaviors into one of 5 categories: (1) pre-contemplation; (2) contemplation; (3) preparation; (4) action; and (5) maintenance.
At month 6, repeat anthropometrics, laboratory studies, and surveys were conducted. Follow-up measures were limited by the impact of the COVID-19 pandemic that restricted in person research visits and data collection. Participants received a $25 gift card for each study visit completed. Procedures of the study were approved by the University of Michigan Institutional Review Board and all participants provided informed written consent prior to the study. All methods were performed in accordance with relevant guidelines and regulations. This study was first registered in clinicaltrials.gov on 12/02/2019 (NCT03839082). Results of the study are reported in accordance with the CONSORT 2010 guidelines.
Lifestyle intervention
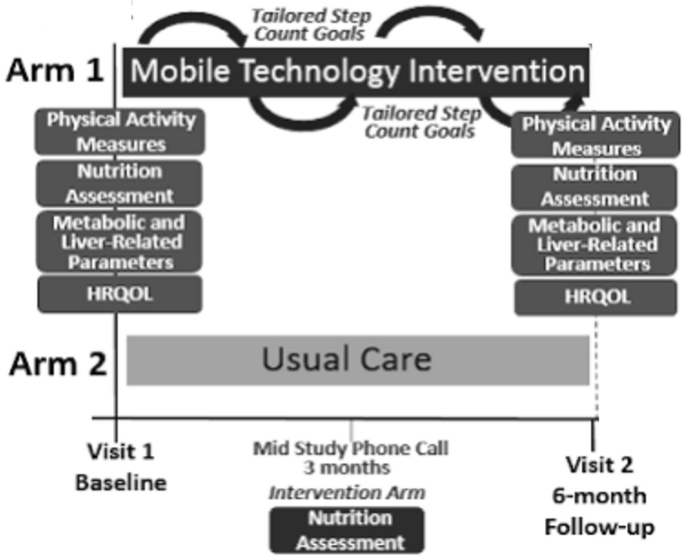
Patients were randomized to either usual care in the general hepatology clinic or to mobile-technology based intervention for 6-months (Fig. 1). At our center, usual care for patients with NAFLD without decompensated cirrhosis consists of visits every 6–12 months. Visits are approximately 15–20 min and consist of review of weight, recent laboratory tests and VCTE/imaging if ordered. Management typically consists of a brief overview of lifestyle changes including improvements in nutrition and physical activity. Patients in usual care did not consistently receive specific educational materials nor dietician evaluation. Vitamin E is prescribed in a small proportion of patients. A similarly small proportion of patients are formally referred to and subsequently evaluated by a nutritionist.
Mobile-technology based intervention compared to usual care.
The mobile technology-based lifestyle intervention design was informed by our prior pilot trial7. Participants in the intervention arm received a Fitbit Zip at enrollment to track step counts. The Fitbit wirelessly syncs data from the tracker to the Fitbit software or app. Study staff assisted with downloading the software and instructed participants to wear their FitBit during waking hours every day. At any time if the participant had questions or problems regarding the use of the FitBit, a study staff member could be contacted.
Study staff retrieved users’ step count data for analysis weekly and provides subjects with personalized feedback on step counts with tailored goals (10% increase per week with maximum increase of 800 steps per week to a maximum of 10,000 steps/day) and motivational messaging based on their prior step count and nutritional evaluation via e-mail. These goals were modeled after the United States Preventative Services Task Force (USPSTF) recommendations for physical activity14. Patients with consecutive days without data recorded or with other signs of low FitBit usage (days with minimal step counts) were contacted by study staff via e-mail or phone if necessary to encourage use. Feedback occurred weekly for the first 3 months and then biweekly for another 3 months. Patients in the intervention arm also had a nutritional assessment by a nutritionist specialized in NAFLD at enrollment. As part of the longitudinal feedback e-mails, patients were also asked about progress with diet/nutrition. Participants in the intervention arm also received our NAFLD educational folder that included: (1) NAFLD disease information including diagnosis, clinical manifestations, natural history and treatments; (2) NAFLD nutritional recommendations including sample menus; (3) NAFLD physical activity recommendations including walking programs and physical activity logs; (4) weight tracking logs; and (5) resources for diet and exercise programs15. Participants were encouraged to incorporate physical activity beyond walking. Data on types of physical activity completed by the participant on a regular basis were captured in the IPAQ assessments.
Outcomes of interest
The outcomes included correlates of lifestyle behaviors and HRQOL, and improvements in metabolic and liver-related clinical parameters, HRQOL, and physical activity patterns at month 6 after implementation of our mobile technology intervention. Due to COVID-19 pandemic restrictions on in-person clinic and research visits, follow-up data was restricted to survey data which limited the pre/post analyses of the impact of the intervention.
Statistical analysis
To assess baseline characteristics and impact of the intervention on outcomes of interest we performed descriptive and bivariate analyses. For descriptive statistics, medians and interquartile ranges (IQR) for continuous data and frequencies and percent for categorical data are presented. Correlations between lifestyle patterns and variables of interest were determined by univariate and multivariate linear and logistic regression. Candidate variables for multivariate analyses were selected based on results of univariate analysis, biologic plausibility and results of prior published studies. End of intervention analyses were assessed using the Wilcoxon rank-sum test to evaluate differences in medians given the small sample size and wide distribution of data points in the cohort. P values < 0.05 were considered statistically significant. All analyses were performed in STATA 14 (StataCorp, College Station, TX).
link


:max_bytes(150000):strip_icc()/LWWD-Crispy-Peanut-Butter-Quinoa-Balls-Beauty-1x1-0085c48b485b4245a188665577a0e476.jpg "10+ Sweet Diabetes-Friendly Snack Recipes")


